

A field biomed contractor covering five states lives out of a service van, and the schedule rarely bends to fit a classroom in another time zone. Adding ophthalmic devices to that route looks profitable on paper, right up until you hit the training gap, because nobody hands out phaco system credentials at a weekend seminar. The realistic path is remote, which is why surgical eye equipment training that runs on demand keeps drawing contractors who bill by the call. A weak course wastes a week you could have spent billing, while the right one pays for itself almost immediately.
Match Curriculum To The Systems You Service
Start with the nameplate on the machines you actually expect to touch. If your target surgery centers run Alcon Centurion consoles, a generic biomedical refresher does nothing for you, while a course built around that exact platform does the whole job. The money math behind that decision backs this up. A January 2026 coding change trimmed the surgeon fee for CPT 66984 by 11%, and that cut is nudging centers toward in-house maintenance over premium service contracts. That shift is the exact gap a trained field contractor steps into. So match the syllabus to your book of business before you match it to your curiosity. In practice the courses worth your time keep alumni access open, because firmware revisions move and a static training PDF ages fast.
- Which console generations and software revisions does the curriculum actually cover?
- Do I keep access to the material after I finish, or does the portal expire?
- What hands-on component ships with the course, a real toolkit or just video?
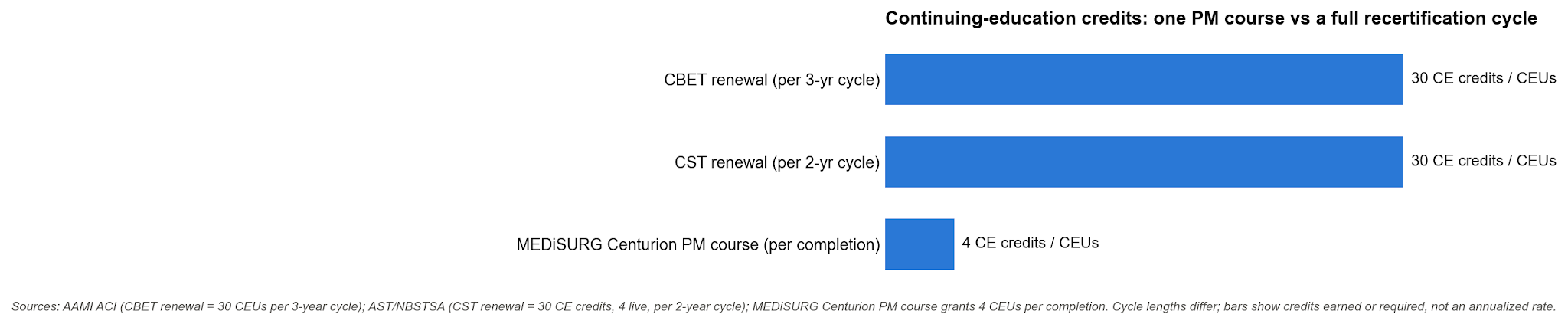
- How many continuing education credits does completion grant, and will my certifying board accept them?
Look For Real Handpiece And Fluidics Modules
A course title can promise phaco coverage and still skip the parts that fail in the field. Fluidics and the handpiece are where preventative maintenance actually lives, so a module list that folds them into one vague overview paragraph should stop you cold. The procedure volume behind it is the reason this matters. JAMA Ophthalmology counted 2,298,446 routine cataract procedures in Medicare ambulatory surgery centers in a single reported year. Every one of those cases cycles the handpiece and fluid pathways a technician has to keep inside spec. The case we see most often is a contractor who can swap a console board without blinking but freezes on a handpiece that will not tune. The course glossed the tuning routine in a single slide, and it shows the first time real pressure is on. Look for a curriculum that breaks out system overview, eye anatomy, the cataract procedure, troubleshooting, and handpiece configuration as their own blocks. That granularity (dull to skim on a syllabus, I know) is the tell that the training was built by someone who has actually turned wrenches on the equipment.
Confirm Continuing Education Credits Transfer
Credits only help if the board that certifies you actually counts them. A solid PM course might grant four CEUs, yet a Certified Biomedical Equipment Technician renewal and a surgical tech renewal each run on their own cycle with their own required totals. Before you enroll, pull up your certifying board’s public CE registry and confirm the provider is recognized there. AAMI’s Credentialing Institute is the free portal biomed techs check for CBET activities, and it settles the question in a couple of minutes.
Read the fine print on how the credit posts, too. Some providers issue a certificate you have to self-report, while others file the hours directly with your board. That small difference decides whether logging the credit is one email or one lost afternoon of paperwork.
Weigh Self-Paced Access Against Fixed Schedules
Here is where the traveling contractor and the hospital-based tech really split. A staff technician can block a Tuesday for a live cohort, but a contractor billing by the service call cannot afford a fixed webinar that collides with a job three states over. Self-paced on-demand access solves that, and the better programs let you open a module in a hotel parking lot at night and finish it in a break room the next morning. Watch the difference between true self-paced and time-boxed self-paced, though, because some vendors hand you thirty days of access and then quietly lock the portal. Indefinite access matters more than it first sounds, because the first time you hit an unfamiliar fault code, reopening the troubleshooting module beats calling a peer who might be scrubbed in mid-procedure. A course you can pause and resume around real work beats a rigid two-day class that costs you two billable days on the road. That single trade-off is most of the reason remote formats took over this corner of biomedical training.
The Right Program Pays Back Its First Service Call
Total up what the specialty adds before you flinch at the tuition. One new ophthalmic account on a five-state route can mean several service calls a quarter you simply were not billing before, and the course price lands somewhere under a single good invoice. That is the honest test of surgical eye equipment training built for field work, since it should earn back its own cost on the first service call it qualifies you for, then keep paying every quarter after. So pick the course that matches your consoles, teaches the handpiece and fluidics for real, carries credits your board accepts, and stays open on demand. The van does not stop moving, and a program that respects that is the one worth buying.




